
")
Video Chats With Doctors Can Save Lives in Rural Areas
February 10, 2020 | Corinne Boyer | 6 min read
GARDEN CITY, Kansas — When Christi Graber checked into the St. Catherine Hospital emergency room late last year, she thought she was having a heart attack.
Her left arm ached, she felt dizzy, and she experienced shortness of breath.
The hospital’s cardiologist wasn’t available that night or for the next three days, so Graber had two options: Travel by ambulance to see a cardiologist more than two hours away in Hays during a snowstorm; or simply go home. Ultimately, she and her husband drove home.
They worried both about the weather and the cost.
“That’s a huge expense to be taken by ambulance a few hours away,” Graber said.
Even the largest hospitals in the rural counties of western Kansas struggle to hire cardiologists and other specialists. Instead, they often transfer patients to Wichita, Denver or Kansas City.
Now those same hospitals increasingly bring in specialists with virtual hook-ups, beaming in doctors from South Dakota who direct treatment over ever-more-elaborate video calls to emergency rooms in Garden City or Goodland.
Yet for all the solutions telemedicine might offer, its obstacles range from iffy internet connections to uncertainties about insurance coverage to simple technophobia.
Emergency Room Telemedicine
If someone suspects they are having a stroke or heart attack, getting to an emergency room in time is critical.
But a visit to a rural emergency room that doesn’t have a cardiologist or neurologist can lead to a transfer by ambulance or air to a metropolitan-area hospital with specialists on hand.
Several frontier counties — areas that have less than six people per square mile — comprise the northwest corner of Kansas. Two critical access hospitals serving the area, Rawlins County Health Center and Goodland Regional Medical Center, have tailored their emergency rooms for telemedicine.

St. Catherine Hospital Emergency Room Director Dora Leon uses a computer to call a neurologist to consult on a patient who might be having a stroke. (Corinne Boyer | Kansas News Service)
Goodland Regional Medical Center and Rawlins County Health Center both contract with Avera eCARE, a virtual hospital that works with 22 critical access hospitals in Kansas. When doctors in those hospitals need more expertise, they connect by video to Avera’s specialists.
Ronald Robinson, a physician and CEO of the Goodland and Rawlins County hospitals, said pulling in the right specialists can make all the difference in a complicated case. Telemedicine, he said, makes that more practical.
“The physician…can see the (electrocardiogram), see the monitor, see the patient and assist us in making sure that we’ve got that correct diagnosis,” Robinson said.
Doctors working remotely with ER patients can also assist bedside nurses and doctors with procedures, such as guiding them on putting in a breathing tube. Robinson said cameras mounted in emergency rooms allow doctors to see hospital equipment and walk staff through the process.
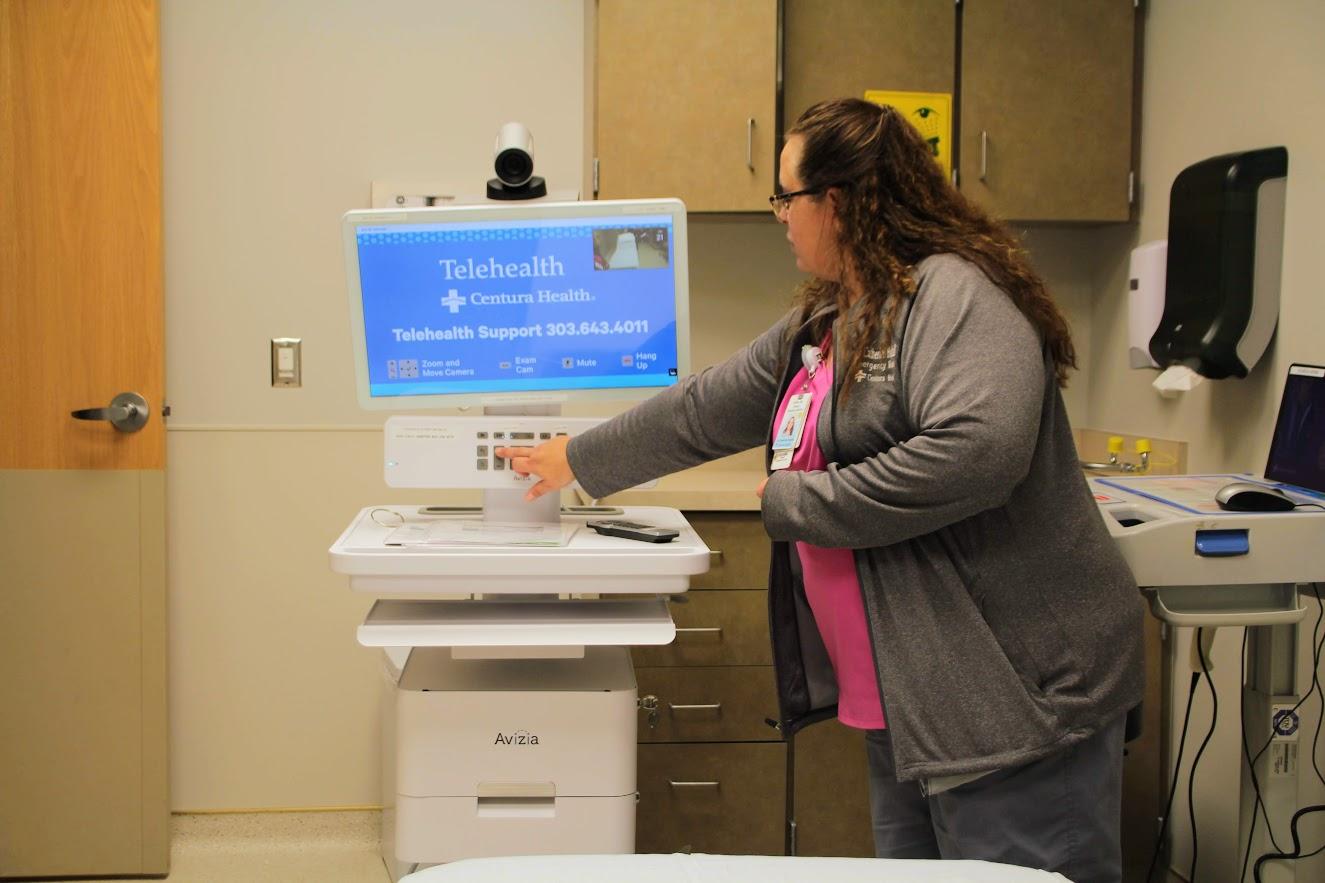
To begin a telemedicine call, someone simply presses a button.
“Directly above that,” said Brian Skow, an emergency medicine specialist and the chief medical officer of Avera eCARE, “there’ll be a 55-inch high-definition monitor and then a camera that’s attached to that to access our system.”
The Avera physician appears on the screen in 30 seconds or less, Skow said. Heart attack and stroke calls rank among the most frequent.
“We can determine if it truly is just stroke,” Skow said. “I can read the CAT scan of the brain so I can determine, yes, this would meet criteria for (a) clot-busting drug.”
Finally, the telemedicine service can assist with patients needing further treatment at trauma centers by arranging helicopter, ambulance and plane transfers.
At St. Catherine Hospital in Garden City, if an emergency room patient shows signs of a stroke, a mobile cart with a camera and computer screen wheels a remote neurologist in to examine the patient.
“So if we have that accessibility,” said Dora Leon, a nurse who manages the emergency room at St. Catherine, “that makes us feel more comfortable knowing that if our ER doctor wants a little bit of backup, it’s there. It’s available.”
She said the mobile cart is placed at the foot of a patient’s bed so the neurologist sees the entire body when looking for signs of weakness.
The neurologist can view a patient’s medical information on another screen.
“We hold their arm up, and see how long they can hold it up. (Then), their leg. It’s just to check which side of the brain is affected by the stroke,” Leon said.
All the while, a neurologist, the sort of specialist that St. Catherine doesn’t have on staff, can examine the patient in those critical early moments when a possible stroke has been detected. And when the right treatment matters most.
Virtual Specialists
Based in South Dakota, Avera eCARE works in 16 states in more than 200 hospitals — stretching from Vermont to Texas.
Avera also employs specialists who work remotely with schools, jails and monitor intensive care patients. Doctors who work for the telemedicine company also rotate through Sioux Falls-area hospitals to keep their skills sharp.
St. Catherine Hospital Emergency Room Director Dora Leon positions a telemedicine cart at the foot of a hospital bed. (Corinne Boyer | Kansas News Service)
Physicians must be certified in the state where they work and the states where their telemedicine links take them. They also need credentials in the individual hospitals that hire telemedicine contractor.
In 2018, the Kansas Legislature passed a bill expanding telemedicine by requiring insurance companies to cover treatment given over video hook-ups as if it were delivered in person.
Robinson said that, in turn, has given small hospitals like Goodland and Rawlins County more incentive to pay for dedicated internet lines and tap into some federal subsidies for those connections.
Yet obstacles remain. Some telemedicine rules remain uncertain.
“An insurance plan must provide coverage for telemedicine services, but it does not require that insurance company to pay the same as it would for the in-person visits,” said Jennifer Findley of the Kansas Hospital Association.
That means hospitals can be unsure how much reimbursement they get from insurance companies for care involving telemedicine.
Meanwhile, Findley said, reliable broadband isn’t wired into every rural hospital in the state.
“We have (some) places where it’s still challenging to get a dedicated connection,” she said.
Even when the billing might be clear and the internet steady, hospital administrator can find themselves worried about what it costs to start up telemedicine or whether a small outfit can muster a plan.
Janine Gracy assesses hospitals’ technology and organization for the Heartland Telehealth Resource Center. She says some facilities are more intimidated than they should be.
“If you have a smartphone, if you have an iPad, if you have a laptop, if you have a desktop with a camera and speakers, you can do telemedicine,” she said. “You don’t have to go out and buy a robot in order to offer telemedicine.”
Corinne Boyer covers western Kansas for High Plains Public Radio and Kansas News Service.
Reading these stories is free, but telling them is not. Start your monthly gift now to support Flatland’s community-focused reporting.

Related Stories

Nick’s Picks | Messi, Jail, Buses, and More …
World Cup Team(s) Arrive It’s starting to feel real. The first World Cup team has landed in Kansas City. Defending champions Argentina touched down at KCI airport on Sunday and will begin practicing today at Sporting KC’s training facility in Wyandotte County. Much of the attention, of course, is focused on Lionel Messi. The soccer…

World Cup ‘Statement Piece’ Evokes Best Version of Kansas City
Before I moved to Kansas City almost 56 years ago, I had been here only once — for a brief visit to the Kansas City Press Club when I was attending the University of Missouri School of Journalism. But because of that visit and the fact that I grew up in the Midwest (Woodstock, Illinois,…

KU Center Helps Women Gain Foothold After Incarceration
A flier from her probation officer was the turning point for Jodi Whitt, who had spent more than two decades in and out of the criminal justice system. The piece of paper introduced Whitt to the Technology Education Program offered by the University of Kansas’ Center for Digital Inclusion. Since 2019, Whitt has risen through…